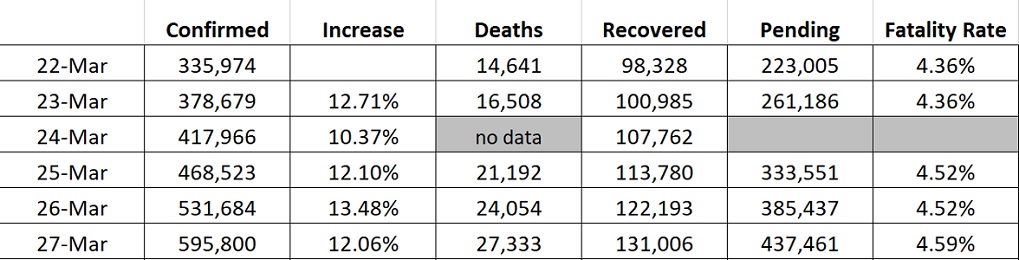
Someone at John Hopkins flunked remedial math. 27,333/(27,333+131006) = 17.2%.
He didn't "flunk remedial math"; he's describing the death rate as a percentage of
confirmed cases.
27,333/595,800 = 4.59%
Now, as to whether that's the computation he
should be using...that's a different matter!
Actually, I think
neither one is the correct computation.
A More Meaningful Computation
A
better (though still imperfect) computation to use would be to find out the mean time from infection to death (for cases in which death is the outcome), and then
backtrack to find the number of confirmed cases
that many days ago.
So if there were 27,333 deaths today, and they all got infected roughly 2 weeks ago, and if 2 weeks ago there were 485,702 confirmed cases, then the real percentage would be 27,333/485,702 = 5.6%.
After all, it's neither cases that were just confirmed today, nor the sum of cases resolved today (dead+recovered) that produces an eventual death in a still-active case. It's the infecting of
that case that eventually leads to
that death.
That's what the computation I'm proposing, above ^^^ would give us.
A Further Caveat
Of course all this is
still not correct, because the "Confirmed Active Cases" on any given day is underestimating the
real number of Active Cases by an unknown multiple between 5 and 20. (I use "5 and 20" because those are the lowest and highest estimates I've seen for the number of infections we're missing due to lack of testing. Two weeks ago it was probably closer to 20; hopefully with increased testing it'll be coming downwards.)
So in reality, if 2 weeks ago we tested people and got 485,702 confirmed infections, the
actual number of infections was somewhere between 2.4 million and 9.7 million. And that would put the eventual deaths from
those infections as somewhere between 1.1% and 0.2%.
P.S. While I was typing this, I see that somebody else came in pointed out how the Johns Hopkins number was calculated. Sorry to be redundant in pointing that out.